
Artroplastia total de cadera de doble movilidad en fracturas del cuello femoral. Estudio prospectivo multicéntrico de 131 casos con seguimiento mínimo de 1 año.
Dual Mobility Total Hip Arthroplasty to treat femoral neck fracture. A prospective multicentre study of 131 cases at a minimum follow up of 1 year
Jean Louis Prudhon 1, André Ferreira 2, Jean Marc Puch 3, Loys Descamps 3, Régis Verdier 4
1 Centre ostéo articulaire, Echirolles, 2 Clinique du Parc, Lyon, 3 Clinique Saint-Georges, Niza, 4 Genay Cedex, Francia
1 Centre ostéo articulaire, Echirolles, 2 Clinique du Parc, Lyon, 3 Clinique Saint-Georges, Niza, 4 Genay Cedex, Francia
Autor para correspondencia:
Dr. Jean-Louis Prudhon
Centre ostéo articulaire. 5 Rue des tropiques 38130 Echirolles, France
E-mail: jean-louis.prudhon@wanadoo.fr
Dr. Jean-Louis Prudhon
Centre ostéo articulaire. 5 Rue des tropiques 38130 Echirolles, France
E-mail: jean-louis.prudhon@wanadoo.fr
Resumen
Objetivo: Cada año se contabilizan en Francia más de seis mil fracturas de cuello de fémur (FNF). La hemiartroplastia (HA) es el tratamiento más frecuente aunque la artroplastia total de cadera (THA) es una buena opción. Sin embargo, la luxación es un problema frecuente y el cotilo de doble movilidad (DMC) es eficaz para prevenir la luxación. El objetivo del presente trabajo es analizar las luxaciones y otro tipo de complicaciones, basado en un estudio multicéntrico, de prótesis totales con un DCM, en pacientes mayores con FNF, un año después de su colocación.
Material y metodología: Estudio multcéntrico. Se recogieron los datos de seis hospitales franceses en un registro privado. De mayo 2012 a junio 2016 se operaron 131 casos (129 pacientes) consecutivos, con vástagos femorales sin cementar (52,7%) o cementados. El cotilo DMC se fijó sin cementar en todos los casos. Once pacientes (8,5%) fallecieron en este periodo por causas desconocidas, 2 (1,7%) se perdieron durante el estudio.
Resultados: En un paciente se luxó su prótesis 11 días después de la cirugía que se redujo sin ningún problema. No hubo recurrencia posterior. Otro paciente presentó 7 días después de la intervención una luxación debido al hundimiento del vástago femoral.
Conclusión: La luxación es el mayor problema en las THA. La DMC es, para nosotros, la mejor solución. Nuestra serie demuestra el bajo índice de luxación (0,84%) que coincide con publicaciones anteriores. Según nuestra experiencia, la DMC es la opción más interesante para tratar FNF en pacientes de edad elevada.
Material y metodología: Estudio multcéntrico. Se recogieron los datos de seis hospitales franceses en un registro privado. De mayo 2012 a junio 2016 se operaron 131 casos (129 pacientes) consecutivos, con vástagos femorales sin cementar (52,7%) o cementados. El cotilo DMC se fijó sin cementar en todos los casos. Once pacientes (8,5%) fallecieron en este periodo por causas desconocidas, 2 (1,7%) se perdieron durante el estudio.
Resultados: En un paciente se luxó su prótesis 11 días después de la cirugía que se redujo sin ningún problema. No hubo recurrencia posterior. Otro paciente presentó 7 días después de la intervención una luxación debido al hundimiento del vástago femoral.
Conclusión: La luxación es el mayor problema en las THA. La DMC es, para nosotros, la mejor solución. Nuestra serie demuestra el bajo índice de luxación (0,84%) que coincide con publicaciones anteriores. Según nuestra experiencia, la DMC es la opción más interesante para tratar FNF en pacientes de edad elevada.
Abstract
Purpose: More than sixty thousand femoral neck fractures (FNF) occurred in France each year. Hemiarthroplasty (HA) is the most common treatment used. Total hip arthroplasty (THA) is a merging option. However, dislocation remains the main issue. Dual mobility cup (DMC) has demonstrated its efficiency to prevent dislocation. Based on a prospective multicentre study, the purpose of this study, is to analyse dislocation rate at 1 year and the causes for revision.
Material and Methodology: Six Private French Orthopaedic Institutions have collected data in a prospective and exhaustive manner in a private register. From May 2012 to June 2016, 131 consecutive cases (129 patients) have been included. Femoral implants were cementless (52.7%) or cemented. The contemporary DMC is made of cobalt–chromium–molybdenum alloy. Fixation was obtained by cementless fixation in all cases.
Results: Eleven patients (8.5%) died of unrelated causes, 2 (1.7%) are lost to follow up. One patient has dislocated her hip 11 days after surgery. Dislocation was closely reduced. No recurrence has occurred. One patient has presented 7 days after surgery a dislocation due to a subsidence of the cement less femoral component.
Conclusion: Dislocation is the main issue of THA. DMC is, for us, the best solution. Our series has demonstrated a rate of dislocation of 0.84% which is consistent with that of previously reported. According to our experience, we can assess that DMC THA is the most relevant option to treat FNF in the elderly population.
Material and Methodology: Six Private French Orthopaedic Institutions have collected data in a prospective and exhaustive manner in a private register. From May 2012 to June 2016, 131 consecutive cases (129 patients) have been included. Femoral implants were cementless (52.7%) or cemented. The contemporary DMC is made of cobalt–chromium–molybdenum alloy. Fixation was obtained by cementless fixation in all cases.
Results: Eleven patients (8.5%) died of unrelated causes, 2 (1.7%) are lost to follow up. One patient has dislocated her hip 11 days after surgery. Dislocation was closely reduced. No recurrence has occurred. One patient has presented 7 days after surgery a dislocation due to a subsidence of the cement less femoral component.
Conclusion: Dislocation is the main issue of THA. DMC is, for us, the best solution. Our series has demonstrated a rate of dislocation of 0.84% which is consistent with that of previously reported. According to our experience, we can assess that DMC THA is the most relevant option to treat FNF in the elderly population.
: Cadera, Prótesis total cadera, Cotilo, Luxación, Fractura cuello fémur
: Hip, Total hip arthroplasty, Cup, Dislocation, Femur neck fracture
Introducción
More than sixty thousand femoral neck fractures (FNF) occurred in France each year. Arthroplasty seems the most relevant option to treat displaced FNF in the elderly population.
Hemiarthroplasty (HA) is the most common treatment used as reported by several authors [1,2] and largest National Hip Arthroplasty Register [3-5]. Total hip arthroplasty (THA) is a merging option since 2 decades to address the issue of post-operative pain and low functional results reported with hemiarthroplasty [6-14]. Even though, THA vs HA mortality rate at 1 year is the same [11].
Burgers [9] in a meta-analysis including 8 randomized trial controls (RCT) with a total of 986 patients has compared HA versus THA to treat displaced FNF. He has demonstrated that in THA, post-operative pain and revision rate is lower than in HA (4% versus 7%). Yu [10] has reported the same results. However, dislocation remains the main issue with standard THA [11]. Risk factors are higher in this population than patients operated on for primary osteoarthritis.
Dual mobility cup (DMC) has demonstrated its efficiency to prevent dislocation in high risk patients. [15-18]. Based on a prospective multicentre study of 131 displaced FNF treated by DMC, the purpose of this study, is to analyse dislocation rate at 1 year and the causes for revision within the first year of follow up.
Hemiarthroplasty (HA) is the most common treatment used as reported by several authors [1,2] and largest National Hip Arthroplasty Register [3-5]. Total hip arthroplasty (THA) is a merging option since 2 decades to address the issue of post-operative pain and low functional results reported with hemiarthroplasty [6-14]. Even though, THA vs HA mortality rate at 1 year is the same [11].
Burgers [9] in a meta-analysis including 8 randomized trial controls (RCT) with a total of 986 patients has compared HA versus THA to treat displaced FNF. He has demonstrated that in THA, post-operative pain and revision rate is lower than in HA (4% versus 7%). Yu [10] has reported the same results. However, dislocation remains the main issue with standard THA [11]. Risk factors are higher in this population than patients operated on for primary osteoarthritis.
Dual mobility cup (DMC) has demonstrated its efficiency to prevent dislocation in high risk patients. [15-18]. Based on a prospective multicentre study of 131 displaced FNF treated by DMC, the purpose of this study, is to analyse dislocation rate at 1 year and the causes for revision within the first year of follow up.
Material y metodología
Six Private French Orthopaedic Institutions in Grenoble, Lyon, Nice have collected data in a prospective and exhaustive manner in a private register [15]. Data were collected with an electronic case report form which allow to ensure the study procedures are being followed and to carry out real-time statistical analyses (OrthoWave software, https://web.orthowave.net/). The confidentiality and data security protocol were approved by the French Advisory Committee on Information Processing in Material Research in the Field of Health (CCTIRS) and the “Commission Nationale Informatique et Liberté” (CNIL: French data protection act, https://www.cnil.fr/en/home)
The patients have signed a consent that allows encoding data to be included and used for research purposes.
From May 2012 to June 2016, 131 consecutive cases (129 patients) operated on for THA to treat FNF have been included. We have limited this evaluation to a single product line of a contemporary DMC, available as cemented and cementless versions named QUATTROä Dual Mobility Cup (Groupe Lepine, Genay, France) (Figure 1).

The patients have signed a consent that allows encoding data to be included and used for research purposes.
From May 2012 to June 2016, 131 consecutive cases (129 patients) operated on for THA to treat FNF have been included. We have limited this evaluation to a single product line of a contemporary DMC, available as cemented and cementless versions named QUATTROä Dual Mobility Cup (Groupe Lepine, Genay, France) (Figure 1).
Figure 1. Quattro Dual Mobility Cup (DMC). Quattro®-cup cementless 1A: VPS HA; 1B press fit; 1C: cemented cup.
This DMC is made of cobalt–chromium–molybdenum alloy. Fixation can be obtained by cementation or by a cementless fixation. The primary fixation is obtained by an outer macrostructure: 6 equatorial fins and 4 tropical spikes. Mid and long-term fixation is obtained by bilayer coating of vacuum-plasma sprayed pure porous titanium and hydroxyapatite. The inner surface of the cup is highly-polished. The liner is machined from standard Ultra-High Molecular Weight Polyethylene (UHMWPE) sterilized by ethylene oxide.
Patient characteristics: age, gender, BMI, ASA score, type of fracture according to Garden classification [16].
Surgical data: surgical approach such as posterior-lateral, anterior lateral Hardinge, direct anterior approach. Femoral implants (Groupe Lépine, Genay, France) were cementless implants: PAVIä, TARGOSä, MINI TARGOSä, EXEL Rä or cemented: INSTITUTIONä. Femoral necks were highly polished (roughness of 0.1µm) Femoral head diameter were 22.2 or 28 mm in stainless steel or 28 mm in ceramic.
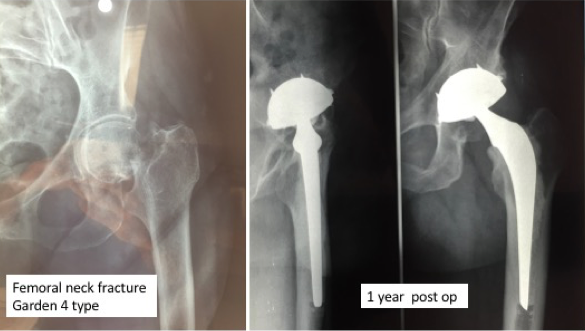
Clinical scores (PMA, HSS) and radiological (Figure 2) analysis based on a standard regular follow-up of 3 months, 1 year, 2 years and then every 2 years. Any intra-operative or postoperative complications are recorded.
Patient characteristics: age, gender, BMI, ASA score, type of fracture according to Garden classification [16].
Surgical data: surgical approach such as posterior-lateral, anterior lateral Hardinge, direct anterior approach. Femoral implants (Groupe Lépine, Genay, France) were cementless implants: PAVIä, TARGOSä, MINI TARGOSä, EXEL Rä or cemented: INSTITUTIONä. Femoral necks were highly polished (roughness of 0.1µm) Femoral head diameter were 22.2 or 28 mm in stainless steel or 28 mm in ceramic.
Clinical scores (PMA, HSS) and radiological (Figure 2) analysis based on a standard regular follow-up of 3 months, 1 year, 2 years and then every 2 years. Any intra-operative or postoperative complications are recorded.
Figure 2.Femoral neck fracture Garden 4 treated by THA. Cementless DMC with cemented Charnley femoral component.
The main characteristics of the series are consistent with similar series reported on FNF (Table 1). Two third of the patients were females, mean age at surgery was 79 years. One patient on 2 was ASA III and IV. Postero lateral approach with capsular repair has been used in most of the cases. Femoral component was uncemented in 52.7% of the cases. The acetabular component was uncemented in all the cases (Table 1).
Statistical analysis: Qualitative variables are presented as percentage, quantitative variables as mean and range.
Statistical analysis: Qualitative variables are presented as percentage, quantitative variables as mean and range.
Table 1 – Patients demography and implant characteristics
| Mean age (range) years | 79 (44-99) |
| Sex | 65% women |
| Mean BMI (range) (kg/m²) | 25.3 (17-35) |
| ASA | |
| I | 6.3 |
| II | 39.7 |
| III | 47.6 |
| IV | 6.3 |
| Surgical approach (%) | |
| Posterior | 94.4 |
| Hardinge | 5.6 |
| Femoral stems, (%) | |
| Cemented | 31 |
| Cementless | 69 |
| Acetabular cup, (%) | |
| Quattro cup – cemented | 0 |
| Quattro cup – cementless VPS HA | 43.5 |
| Quattro cup – cementless press-fit | 56.5 |
| Acetabular cup size, (%) | |
| 44 | 3.3 |
| 46 | 18.7 |
| 48 | 19.5 |
| 50 | 25.2 |
| 52 | 17.1 |
| 54 | 11.4 |
| 56 | 2.4 |
| 58 | 2.4 |
Resultados
Among the 129 patients recorded in our data base 11 patients (8.5%) died of unrelated causes and 2 patients (1.7%) are lost to follow up. Two patients (1.7%) were revised for early peri-prosthetic femoral fracture.
One patient (90 years old female) have dislocated her hip (cemented femoral component + cementless Quattro cup) 11 days after surgery due to a fall. Dislocation was closely reduced. No recurrence has occurred.
One patient (80 years old female) has presented 7 days after surgery a dislocation due to a subsidence of the cement less femoral component. An intra operative fracture probably occurred and was unknown at the time of surgery. This patient was revised with a cementless long stem with 2 distal locking screws.
One patient (77 years old female) has presented 1 month after surgery a peri-prosthetic femoral fracture (Vancouver B 2). It was treated by femoral revision with a long cementless femoral implant.
One patient (95 years old female) has presented 2 years after surgery (THA +TKA) an inter-prosthetic fracture of the femur. It was treated by open reduction and internal fixation with a long locking plate.
If we exclude the patient that has presented a dislocation due to the femoral subsidence, no patients were revised for dislocation.
No prosthetic joint infection has occurred in this series.
Two sciatic nerve palsy were observed. At one year follow up the patients totally recovered.
One patient (90 years old female) have dislocated her hip (cemented femoral component + cementless Quattro cup) 11 days after surgery due to a fall. Dislocation was closely reduced. No recurrence has occurred.
One patient (80 years old female) has presented 7 days after surgery a dislocation due to a subsidence of the cement less femoral component. An intra operative fracture probably occurred and was unknown at the time of surgery. This patient was revised with a cementless long stem with 2 distal locking screws.
One patient (77 years old female) has presented 1 month after surgery a peri-prosthetic femoral fracture (Vancouver B 2). It was treated by femoral revision with a long cementless femoral implant.
One patient (95 years old female) has presented 2 years after surgery (THA +TKA) an inter-prosthetic fracture of the femur. It was treated by open reduction and internal fixation with a long locking plate.
If we exclude the patient that has presented a dislocation due to the femoral subsidence, no patients were revised for dislocation.
No prosthetic joint infection has occurred in this series.
Two sciatic nerve palsy were observed. At one year follow up the patients totally recovered.
Discusión
The treatment of displaced femoral neck fracture in elderly population remains a vast subject of debate. Conservative treatment does not seem recommended [6][7]. HA or THA are the most relevant treatment but specific complications can occur in both surgical option. If we exclude infection, the most frequent complication is dislocation. This complication can be observed in HA with a rate of 14.6% according to Bensen et al. [8]. The other main issue of HA is the functional outcomes that are regularly lower than with THA as reported by Wang et al. [9] and Yu et al. [10].
Holey et al. [11] reported in a systematic literature revue and meta-analysis, that single stage total hip arthroplasty may lead to lower reoperation rates and better functional outcomes compared with hemiarthroplasty in older patients with displaced femoral neck fractures. Macaulay et al. [12,13] in a prospective RCT concluded in the same manner.
Burger et al. [14] stated that THA for displaced FNF in the fit elderly may lead to higher patient-based outcomes but has higher dislocation rates compared with hemiarthroplasty.
Dislocation is the main issue of THA to treat displaced FNF specially when patient’s conditions are poor as frequently observed with this elderly population. Dislocation can be addressed with the use of anterior-lateral approach or direct anterior approach. In our study, most of the cases were operated on by a posterior lateral approach with capsular repair. The dislocation we had reported occurred on a patient operated by posterior-lateral approach.
Large femoral heads are also a solution to prevent dislocation [17]. Metal on metal bearings seem definitively stopped in many countries. Ceramic on Ceramic bearings give excellent results but, due to the over cost, their used is not recommended on this short living expectancy population.
DMC are, for us, the best solution. Our series has demonstrated a rate of dislocation of 0.84% which is consistent with that previously reported [18-20]. In a previous study, we had compared dislocation rate in THA using in one brand a standard cup and in one brand DMC. We have clearly demonstrated that revision rate was significantly lower with DMC even though the population was a higher risk population [21].
Constrained cups have been proposed as an alternative by several authors [22] but in our experience, we only used them to treat DMC failures.
According to our experience related in this study which is consistent with that of has been published in the literature, we can assess that THA using a DMC is the most relevant option to treat FNF in the elderly population or for patients with very poor muscles conditions that may lead to hip dislocation.
Holey et al. [11] reported in a systematic literature revue and meta-analysis, that single stage total hip arthroplasty may lead to lower reoperation rates and better functional outcomes compared with hemiarthroplasty in older patients with displaced femoral neck fractures. Macaulay et al. [12,13] in a prospective RCT concluded in the same manner.
Burger et al. [14] stated that THA for displaced FNF in the fit elderly may lead to higher patient-based outcomes but has higher dislocation rates compared with hemiarthroplasty.
Dislocation is the main issue of THA to treat displaced FNF specially when patient’s conditions are poor as frequently observed with this elderly population. Dislocation can be addressed with the use of anterior-lateral approach or direct anterior approach. In our study, most of the cases were operated on by a posterior lateral approach with capsular repair. The dislocation we had reported occurred on a patient operated by posterior-lateral approach.
Large femoral heads are also a solution to prevent dislocation [17]. Metal on metal bearings seem definitively stopped in many countries. Ceramic on Ceramic bearings give excellent results but, due to the over cost, their used is not recommended on this short living expectancy population.
DMC are, for us, the best solution. Our series has demonstrated a rate of dislocation of 0.84% which is consistent with that previously reported [18-20]. In a previous study, we had compared dislocation rate in THA using in one brand a standard cup and in one brand DMC. We have clearly demonstrated that revision rate was significantly lower with DMC even though the population was a higher risk population [21].
Constrained cups have been proposed as an alternative by several authors [22] but in our experience, we only used them to treat DMC failures.
According to our experience related in this study which is consistent with that of has been published in the literature, we can assess that THA using a DMC is the most relevant option to treat FNF in the elderly population or for patients with very poor muscles conditions that may lead to hip dislocation.
Referencias
- Kim SH, Meehan JP, Lee MA. Surgical treatment of trochanteric and cervical hip fractures in the United States: 2000-2009. J Arthroplasty. 2013; 28:1386-90.
- Hongisto MT, Pihlajamaki H, Niemi S, Nuotio M, Kannus P, Mattila VM. Surgical procedures in femoral neck fractures in Finland: a nationwide study between 1998 and 2011. Int Orthop. 2014; 38:1685-90.
- Australian Orthopaedics Association National Joint Replacement Registry. Annual Report 2012. 2012.
- National Joint Registry for England and Wales. 10th Report. 2013 2013.
- Swedish Hip Arthroplasty Register. Annual Report 2013. 2013
- Blomfeldt R, Törnkvist H, Ponzer S, Söderqvist A, Tidermark J. Comparison of internal fixation with total hip replacement for displaced femoral neck fractures. Randomized, controlled trial performed at four years. J Bone Joint Surg Am. 2005; 87:1680-8.
- Keating JF, Grant A, Masson M, Scott NW, Forbes JFDisplaced intracapsular hip fractures in fit, older people: a randomised comparison of reduction and fixation, bipolar hemiarthroplasty and total hip arthroplasty. Health Technol Assess. 2005; 9:1-65.
- Bensen AS, Jakobsen T, Krarup N. Dual mobility cup reduces dislocation and re-operation when used to treat displaced femoral neck fractures. Int Orthop. 2014; 38:1241-5.
- Wang Z, Bhattacharyya T. Outcomes of hemiarthroplasty and total hip arthroplasty for femoral neck fracture: A Medicare cohort study. J Orthop Trauma. 2017; 31:260-263.
- Yu L, Wang Y, Chen J. Total hip arthroplasty versus hemiarthroplasty for displaced femoral neck fractures: meta-analysis of randomized trials. Clin Orthop Relat Res. 2012; 470:2235-43.
- Hopley C, Stengel D, Ekkernkamp A, Wich M. Primary total hip arthroplasty versus hemiarthroplasty for displaced intracapsular hip fractures in older patients: systematic review. BMJ. 2010; 340:2332.
- Macaulay W, Nellans KW, Garvin KL, Iorio R, Healy WL, Rosenwasser MP; other members of the DFACTO Consortium. Prospective randomized clinical trial comparing hemiarthroplasty to total hip arthroplasty in the treatment of displaced femoral neck fractures: winner of the Dorr Award. J Arthroplasty. 2008; 23(Suppl 1):2-8.
- Macaulay W, Nellans KW, Iorio R, Garvin KL, Healy WL, Rosenwasser MP; DFACTO ConsortiumTotal hip arthroplasty is less painful at 12 months compared with hemiarthroplasty in treatment of displaced femoral neck fracture. HSS J. 2008; 4:48-54.
- Burgers PT, Van Geene AR, Van den Bekerom MP, Van Lieshout EM, Blom B, Aleem IS, et al. Total hip arthroplasty versus hemiarthroplasty for displaced femoral neck fractures in the healthy elderly: a meta-analysis and systematic review of randomized trials. Int Orthop. 2012; 36:1549-60.
- Ferreira A, Prudhon JL, Verdier R, Puch JM, Descamps L, Dehri G, et al. Contemporary dual mobility cup regional and private register: methodology and results. Int Orthop. 2017; 41:439-45.
- Garden RS. Low-angle fixation in fractures of the femoral neck. J Bone Joint Surg (Br). 1961; 43-B:647–63.
- Ricci WM, Langer JS, Leduc S, Streubel PN, Borrelli J Jr.Total hip arthroplasty for acute displaced femoral neck fractures via the posterior approach: a protocol to minimise hip dislocation risk. Hip Int. 2011; 21:344-50.
- Tarasevicius S, Busevicius M, Robertsson O, Wingstrand H. Dual mobility cup reduces dislocation rate after arthroplasty for femoral neck fracture. BMC musculoskeletal disorders. 2010; 11:175.
- Adam P, Philippe R, Ehlinger M, Roche O, Bonnomet F, Mole D, et al. Dual mobility cups hip arthroplasty as a treatment for displaced fracture of the femoral neck in the elderly. A prospective, systematic, multicenter study with specific focus on postoperative dislocation. Orthop Traumatol Surg Res. 2012; 98:296-300.
- Tarasevicius S, Robertsson O, Dobozinskas P, Wingstrand H. A comparison of outcomes and dislocation rates using dual articulation cups and THA for intracapsular femoral neck fractures. Hip international : the journal of clinical and experimental research on hip pathology and therapy. 2013; 23:22-6.
- Caton JH, Prudhon JL, Ferreira A, Aslanian T, Verdier R. A comparative and retrospective study of three hundred and twenty primary Charnley type hip replacements with a minimum follow up of ten years to assess whether a dual mobility cup has a decreased dislocation risk. Int Orthop. 2014; 38:1125-9.
- Hernigou P, Ratte L, Roubineau F, Pariat J, Mirouse G, Guissou I, Allain J, Lachaniette CH. The risk of dislocation after total hip arthroplasty for fractures is decreased with retentive cups. Int Orthop. 2013; 37:1219-23.