
Resumen
Objetivo
Reportar los resultados obtenidos empleando discectomía y nucleoplastia, mediante un abordaje percutáneo no endoscópico, para el tratamiento del dolor lumbar axial mediante dos tecnologías térmicas: láser y radiofrecuencia, en dos años de seguimiento.
Material y métodos
Desde 1993 y hasta 2014, se obtuvieron datos clínicos de 643 pacientes afectados con dolor lumbar axial de dolor discogénico y que fueron intervenidos con 849 discectomías y nucleoplastias percutáneas no endoscópicas. Se establecieron dos grupos de acuerdo con la energía térmica utilizada (Grupo LS: láser Holmium YAG y grupo RF: fuente de
energía de radiofrecuencia de alta frecuencia). En el grupo LS se realizaron 171 procedimientos y 472 en el grupo RF. Se evaluaron los criterios de MacNab y la escala visual analóga en el período prequirúrgico, 12 y 24 meses después de la cirugía.
Resultados
En la muestra total, se obtuvo un 90% de mejoría (excelentes y buenos resultados) según el criterio Macnab. La EVA mostró diferencias estadísticamente significativas entre las pruebas preoperatorias y posoperatorias de cada grupo a los 24 meses de seguimiento (p = 0,000).
Conclusión
La discectomía y nucleoplastia percutánea no endoscópica con láser o radiofrecuencia, en nuestra serie, son técnicas seguras y eficaces en el manejo del dolor lumbar axial discogénico. La tasa de complicaciones fue menor y los resultados fueron mejores con el uso de la radiofrecuencia frente al láser.
Nivel de evidencia: IV
Abstract
Objective: To report outcomes of discectomy and nucleoplasty, through a percutaneous non-endoscopic approach, for treatment of axial lumbar pain using two thermal technologies: laser and radiofrequency, in two years of follow-up.
Material and methods: From 1993 to 2014, we collected data of 643 patients affected with axial lumbar pain from discogenic pain who were intervened with 849 percutaneous non-endoscopic discectomy and nucleoplasty. Two groups were established according to the thermal energy used (Group LS: Holmium YAG laser. Group RF: High frequency radiofrequency energy source). One-hundred seventy-one procedures were performed with laser and 472 with radiofrequency. MacNab criteria and Visual Analogue Scale were evaluated on presurgical period, 12 and 24 months after surgery.
Results: In the total sample, we obtained 90% of improve (excellent and good results). Statistically significant differences were obtained in the pre-op and post-op VAS of each group at 24-month follow-up (p=0.000).
Conclusion: This series shows that percutaneous non-endoscopy disc decompression using either laser or radiofrequency is a safe and effective technique in the discogenic axial lumbar pain management. Complications rate was lower and outcomes were better in RF group compared with LS group.
Level of evidence: IV
Introduction
Despite its high impact on health systems, triggering factor of “discogenic pain” remains undetermined (1). Some studies consider that the increase in inflammatory factors could promote an increase on sensitivity in the existing neurons and an innervation with nociceptive fibers of the nucleus, causing axial pain (2-5).
Alternatives for discogenic pain treatment are as varied as its causes. From conservative medical treatment up to open arthrodesis techniques (6) (7). Recently, minimally invasive spine surgery (MISS) has expanded the range of possibilities to manage disc diseases that are unresponsive to medical treatment. One of the MISS procedures most widely employed in discogenic lumbar pain treatment is thermal decompression (7) (8). This technique consists in placing, through a percutaneous approach, electrodes that transport controlled thermal energy to increase the temperature at intradiscal level, producing nucleus dehydration and ablation of the pain-generating nervous tissues (6). Most fibers using laser (LS) or radiofrequency (RF) as source of heat (7). Temperature effect may be complemented with mechanical discectomy using graspers to achieve a better decompression (8).
Although exact nature of the mechanism of action is not known, discogenic pain relief using thermal and mechanical discectomy and nucleoplastia could be results from two effects. First, effect on nucleus where heat modulates collagen structure thus causing its fibers to shrink and contract and causing evaporation, which in addition to mechanical extraction creates a reduction in disc volume and decompression of nervous structures (9). Second, effect on annulus by high temperatures, which destroy and inhibit the regeneration of nociceptor nervous fibers, diminish genesis of new blood vessel, and help seal annular fissures (10). Such effects are achieved, as long, as heat exceeds the cytotoxic temperature for the annular nerve fibers, which are considered between 42 and 50 °C (11).
In vitro and in vivo studies, has shown that both -LS and RF- reach temperatures required for nervous ablation. Ramirez et al., (12) presented in their research with Holmium an average of 48 °C. For RF, average temperatures reported are: 32 °C (13), 40 °C (14), 45 to 50 °C (6), up to 70 °C (11).
Although in terms of theoretical thermal effect and the effectiveness on patients, both RF and LS, have been reported to be effective (6) (8) (9) (12) (13), their safety margin and degree of complications is still controversial between surgeons. The purpose of the study was to show our outcomes of percutaneous non-endoscopic discectomy and nucleoplasty for discogenic axial lumbar pain treatment using two technologies: laser and radiofrequency.
Methods and Materials
A retrospective study was conducted on patients treated for axial lumbar pain. From 1993 to 2014, we collected data of 643 patients affected with axial lumbar pain from discogenic pain who were intervened with percutaneous non-endoscopic discectomy and nucleoplasty. Study included records of patients treated with percutaneous non-endoscopic thermal therapy whose reason for consultation was an axial lumbar pain and whose final diagnosis was one of following diseases: degenerative disc disease, black disc, disc bulges, annular tear, or contained herniated disc. Diagnosis was made by history, clinical examination, plane and dynamic X-ray and MRI. Also, surgical note should report at least one positive discogenic test (≥5/10). Study excluded medical records of patients with disc disease showing greater than 50% loss of height, a certain degree of segmental instability, radicular pain, as well as medical charts with incomplete data on follow-ups and evaluation criteria. Two groups were established according to the thermal energy used (Group LS: Holmium YAG laser. Group RF: High frequency radiofrequency energy source).
A total of 849 non-endoscopic discectomies were performed in 643 patients. The statistical demographic was 50.3 % (n=324) male and 49.6 % (n=319) female; average age, at surgery was 51 years (SD=12). The youngest patient was 24 years and the oldest was 86 years old.
Surgeries were performed at Reina Sofia Clinic in Bogotá Colombia, by same team of surgeons and using a standardized technique with minor changes throughout the experience. The source of laser energy used was Holmium YAG Laser (Trimedyne Inc. Irvine, CA). The RF electrode employed was Disc-FX Bipolar System (Elliquence, NYC, NY) and a high-frequency-low temperature radiofrequency energy source called Surgimax (Elliquence LLC, NYC) using bipolar mode.
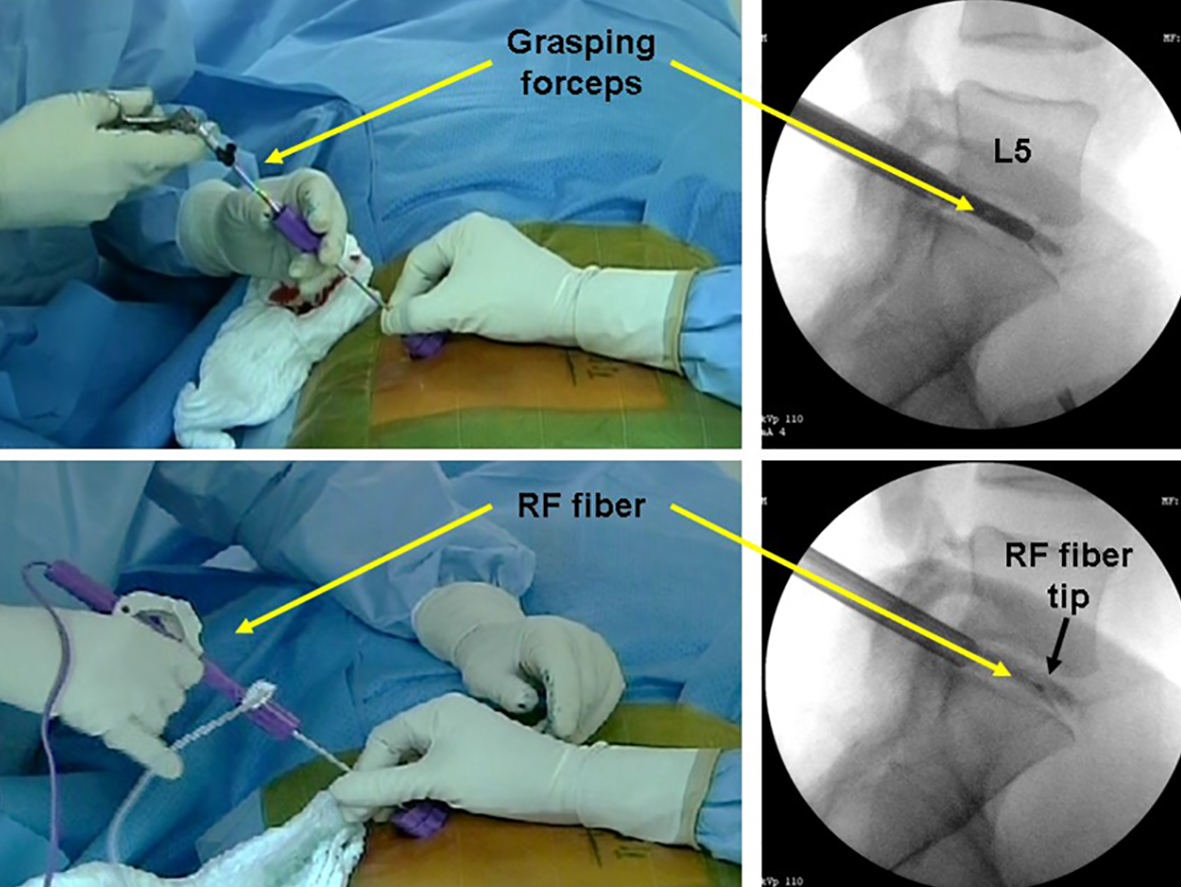
The patient was placed on a prone position. An epidural needle was entered at an angle of 45° with the direction of the foraminal area at a distance between 8 and 12 cm from the midline (figure 1). Needle tip should enter toward posterior third of intervertebral space. Once into intradiscal space, with the aim to reproduce concordant pain, is necessary to do the discography (figure 2). Then, through a sequential system of dilator – cannula - trephine, we perform an annulotomy and thus achieve the nucleus. In order to allow a more extensive decompression, a mechanical resection was performed using grasping forceps (figure 3). Last, electrode was inserted, and thermal discectomy and nucleoplasty was performed (figure 3).
Figure 1. Needle’s angle and point of entry

Figure 2.Discography

Figure 3. Mechanical and thermal discectomy
The evaluation criteria established to determine patient improvement were MacNab modified scale and Visual Analog Scale (VAS). These data were taken directly from the patient, before, tree months after, twelve and twenty four months after the procedure. Medical charts collection and data gathering were conducted by a company independent from the researchers.
Statistical Analysis
Data analysis was performed with the statistical software R 3.1.1 for Windows 8. The analysis determined certain aspects in the variables including frequency and descriptive statistics. The tests selected for comparing the groups were X2 and Wilcoxon for related pairs. The statistical significance was p<0.05.
Results
The most affected levels were L4–L5 and L5–S1, being 73.7% of the total intervened discs (table 1). Whole sample attained 90% satisfactory results and a 4% of complications. The rate of re-operations was 2.5%.
Table 1. Distribution of levels that resulted positive to the discogenic test.
|
Level |
Patients number |
Patients percentage (%) |
|
L1 – L2 |
17 |
2 |
|
L2 – L3 |
53 |
6.3 |
|
L3 – L4 |
154 |
18.1 |
|
L4 – L5 |
329 |
38.8 |
|
L5 – S1 |
296 |
34.9 |
Group LS
Laser technology was employed between March 1993 and January 2007 (13.8 years). 171 medical charts met the inclusion criteria. The number of discs treated in these patients was 207.
Excellent and good (satisfactory) results were obtained in 138 patients (80.7%) in the first 3 months. At the 24-month follow-up, satisfactory outcomes was 83% (n=142) (Table 2). Visual analog scale (VAS) changed from 8.3 (SD=1.34) in the preoperative period to 2.3 (SD=1.80) 12 months after surgery (p=0.000), and to 2.4 (SD=1.64) 24 months after surgery (p=0.000).
Table 2. MacNab Criteria Results
|
3 Months |
12 Months |
24 Months |
||||||||||
|
LS |
RF |
LS |
RF |
LS |
RF |
|||||||
|
Excellent |
122 |
71,3% |
311 |
65,9% |
130 |
76,0% |
421 |
89,2% |
113 |
66,1% |
412 |
87,3% |
|
Good |
16 |
9,4% |
113 |
23,9% |
16 |
9,4% |
18 |
3,8% |
29 |
17,0% |
23 |
4,9% |
|
Fair |
8 |
4,7% |
31 |
6,6% |
0 |
0,0% |
18 |
3,8% |
3 |
1,8% |
18 |
3,8% |
|
Poor |
25 |
14,6% |
17 |
3,6% |
25 |
14,6% |
15 |
3,2% |
26 |
15,2% |
19 |
4,0% |
|
Improvement (E + G) |
138 |
80,7% |
424 |
89,8% |
146 |
85,4% |
439 |
93,0% |
142 |
83,0% |
435 |
92,2% |
There were 18 complications in this sample (10.5%), that is, motor deficit (n=2), one of them definitive with dorsal - flexion paresis (2/5); headache caused by dural sac tear (n=2); post-operative radiculitis (n=8); chemical discitis or vertebral end-plate burning with the laser light (n=4), and infectious spondylodiscitis (n=2).
Group RF
Non-endoscopic discectomies with RF was implemented between January 2007 and March 2014 (7.8 years). A total 472 medical charts met the inclusion criteria and 641 positive discogenic tests were obtained in these patients.
The RF energy showed a satisfactory (excellent–good) result rate of 89.8%, 93.0% and 92.2% when measured at 3, 12 and 24 months, respectively. Regarding pain scale, using RF provided a VAS improvement from 7.9 to 1.8 (p=0.000), at the 24-month follow-up.
There were 8 (1.7%) complications reported by RF use, including transient motor deficit (n=1), headache caused by dural sac tear (n=1), postoperative radiculitis, and infectious spondylodiscitis (n=2).
Discussion
MISS and its benefits—such as a minor trauma in tissues adjacent, less than one-centimeter skin incisions, possibility to employ only local anesthetic and sedation, and early return to work, among others—has been proved on several studies (15-17). Since percutaneous nucleotomy description (18) and its complementing with thermal energy (laser) by Choy and Aschner (19), percutaneous disc decompression procedure has been a procedure implemented in more than 500,000 patients around the world (20). The success of this technique depends greatly on suitable choice of patient, implementation of an appropriate surgical technique, and use of devices that provide greatest safety (8).
In this sample, non-endoscopic discectomy and nucleotomy proved, to two years of follow up, to be a safe and effective technique for treatment of axial lumbar pain caused by a degenerative disc disease, with a high success rate (90%) and a low percentage of associated complications (4%). Different reports have referred to percutaneous disc decompression techniques as replicable, efficient, and effective (7) (20) and have shown results comparable to those presented herein.
Regarding laser technology, Siebert et al., (21) presented a 72.8% success rate in 180 patients at one-year follow-up. Subsequently, Knight and Goswami (22) obtained an improvement in 60% of 576 patients evaluated a year after the procedure. Grönemeyer et al., (23) reported a 75% improvement with 1% of complications in 200 patients. With a smaller sample (37 patients), Black et al., (24) presented an 88% success rate. Also, it is important to mention the outcomes obtained by a pioneer in these techniques, Choy (25) published in 2004 his first 17 years of experience, attaining for MacNab criteria an 89% success rate and a 0.4% complication rate in 1,275 patients (including cervical, thoracic, and lumbar).
There are limited reports about high-frequency-low temperature radiofrequency energy employed by the authors. Hellinger et al., (26) reported an 83% patient satisfaction rate for SF-12 criteria in contained herniated disc and radiculitis, comparable to 90% reported earlier by the same author using MacNab (8) instead and to outcomes attained in this sample. Likewise, Kumar et al., (27) showed a statistically significant improvement from a 6.5 to 3.9 VAS in 12-month follow-up.
To the authors' knowledge, there has not been any publication of percutaneous non-endoscopic discectomy and nucleoplasty using two analog technologies such as LS and RF in the treatment of discogenic axial lumbar pain and neither on the two techniques performed by the same surgeon. Nevertheless, there are comparisons between percutaneous laser disc decompression with LS and microdiscectomy (28) that show little difference in satisfactory results, 83.8% and 85.7% respectively. There are also comparisons of fenestration with same RF using in this series that do not show any statistically significant differences between them (29). Last, a recent randomized controlled trial, comparing percutaneous laser disc decompression with conventional microdiscectomy in sciatica, showed no significant differences between both procedures (9).
It is worth of noting the number of discs actually intervened. For total sample the average was 1.32 discs per patient. Many of additional discs were diagnosed at surgery. For each independent sample, it was determined that for LS the percentage of patients with more than one positive disc was 21% and for RF 36%. Certainly, this difference does not obey to the type of technique, but rather to the experience achieved by surgeons and their understanding of the importance to conduct tests at the adjacent levels, even if there are not any images consistent with disc degeneration.
The percentage of complications in entire sample was 4%, which could be deemed relatively high considering other reports (23) (29) (30). Nevertheless, it is worth of noting that most of the complications occurred in laser experiences, probably due to higher temperatures reached with such technology, but also to their being in the first learning curve phase.
This study has some limitations inherent to observational studies design. We recommended to develop a new study based on a randomized controlled trial design.
As conclusion, we showed in this series that thermal technologies proved, at two years follow up, to be satisfactory in the discogenic axial lumbar pain treatment. Nevertheless, safety margins and occurrence of complications were different.
Conflict of Interest
The authors declare to have received financial support in this research from Elliquence LLC. Dr. Ramírez, Dr. Rugeles, Dr. Ramírez and Dr Prada are consultant for Elliquence. Dr Alonso report no conflicts
References
- Alkhatib B, Rosenzweig DH, Krock E, Roughley PJ, Beckman L, Steffen T, et al. Acute mechanical injury of the human intervertebral disc: link to degeneration and pain. Eur Cell Mater. 2014; 28:98–111.
- Richardson SM, Purmessur D, Baird P, Probyn B, Freemont AJ, Hoyland JA. Degenerate human nucleus pulposus cells promote neurite outgrowth in neural cells. PLoS One. 2012; 7:47735.
- Wuertz K, Haglund L. Inflammatory mediators in intervertebral disk degeneration and discogenic pain. Global Spine J. 2013; 3:175-84.
- Gawri R, Rosenzweig DH, Krock E, Ouellet JA, Stone LS, Quinn TM, et al. High mechanical strain of primary intervertebral disc cells promotes secretion of inflammatory factors associated with disc degeneration and pain. Arthritis Res Ther. 2014; 16:21.
- Miyagi M, Millecamps M, Danco AT, Ohtori S, Takahashi K, Stone LS. ISSLS Prize winner: Increased innervation and sensory nervous system plasticity in a mouse model of low back pain due to intervertebral disc degeneration. Spine. 2014; 39:1345–54.
- Davis TT, Sra P, Fuller N, Bae H. Lumbar intervertebral thermal therapies. Orthop Clin North Am. 2003; 34:255-62.
- Gangi A, Basile A, Buy X, Alizadeh H, Sauer B, Bierry G. Radiofrequency and laser ablation of spinal lesions. Semin Ultrasound, CT MRI. 2005; 26:89–97.
- Hellinger S. Disc-FX. A treatment for discal pain syndromes combining a manual and radiofrequency-assisted posterolateral microtubular decompressive nucleotomy. Eur Musculoskelet Rev. 2011; 6:100-4.
- Brouwer PA, Brand R, van den Akker-van Marle ME, Jacobs WC, Schenk B, van den Berg-Huijsmans AA, et al. Percutaneous laser disc decompression versus conventional microdiscectomy in sciatica: a randomized controlled trial. Spine J. 2015; 15:857-65.
- Finch PM. Radiofrequency denervation of the annulus fibrosus: a rationale. Tech Reg Anesth Pain. 2004; 8:41-5.
- Houpt J, Conner E, McFarland E. Experimental study of temperature distributions and thermal transport during radiofrequency current therapy of the intervertebral disc. Spine. 1996; 21:1808-12.
- Ramirez JF, Rugeles JG. Discolisis percutánea endoscópica lumbar con Holmium YAG Laser. Experiencia de 4 años. Rev Col Ort Trau 2001; 15:57-62.
- Feldman A, Hellinger, S. Disc fx non-endoscopic radiofrequency disc ablation/ decompression/ nucleotomy. First experiences. Internet J Min Inv Spinal Technol. 2006:1(1).
- Ramírez JF, Rugeles JG, Barreto JA, Alonso GO. [Intradiscal temperature variation resulting from radiofrequency thermal therapy. Cadaver study]. Acta Ortop Mex. 2014; 28:12-8.
- Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP et al. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012; 16:452-62.
- Rasouli MR, Rahimi-Movaghar V, Shokraneh F, Moradi-Lakeh M, Chou R. Minimally invasive discectomy versus microdiscectomy/open discectomy for symptomatic lumbar disc herniation. Cochrane Database Syst Rev. 2014; 9:CD010328.
- Ahn Y, Lee SH. Outcome predictors of percutaneous endoscopic lumbar discectomy and thermal annuloplasty for discogenic low back pain. Acta Neurochir (Wien). 2010; 152:1695-702.
- Hijikata S. Percutaneous nucleotomy. A new concept technique and 12 years' experience. Clin Orthop Relat Res. 1989; 238:9–23.
- Choy DS, Ascher PW, Ranu HS, Saddekni S, Alkaitis D, Liebler W, et al. Percutaneous laser disc decompression. A new therapeutic modality. Spine. 1992; 17:949-56.
- Reddy AS, Loh S, Cutts J, Rachlin J, Hirsch JA. New approach to the management of acute disc herniation. Pain Physician. 2005; 8:385–90.
- Siebert WE, Berendsen BT, Tollgaard J. Percutaneous laser disk decompression. Experience since 1989. Orthopade. 1996; 25:42-8.
- Knight M, Goswami A. Lumbar percutaneous KTP532 wavelength laser disc decompression and disc ablation in the management of discogenic pain. J Clin Laser Med Surg. 2002; 20:9-13.
- Grönemeyer DH, Buschkamp H, Braun M, Schirp S, Weinsheimer PA, Gevargez A. Image-guided percutaneous laser disk decompression for herniated lumbar disks: A 4-year follow-up in 200 patients. J Clin Laser Med Surg. 2003; 21:131-8.
- Black W, Fejos AS, Choy DS. Percutaneous laser disc decompression in the treatment of discogenic back pain. Photomed Laser Surg. 2004; 22:431-3.
- Choy DS. Percutaneous laser disc decompression: a 17-year experience. Photomed Laser Surg. 2004; 22:407-10.
- Hellinger S. Treatment of contained lumbar disc herniations using radiofrequency assisted micro-tubular decompression and nucleotomy: four year prospective study results. Int J Spine Surg. 2014 1;24.
- Kumar N, Kumar A, Siddharth S, Sambhav PS, Tan J. Annulo-nucleoplasty using Disc-FX in the management of lumbar disc pathology: Early results. Int J Spine Surg. 2014; 1:18.
- Tassi GP. Comparison of results of 500 microdiscectomies and 500 percutaneous laser disc decompression procedures for lumbar disc herniation. Photomed Laser Surg. 2006; 24:694-7.
- Liao X, Jiang J, Xiong D. The comparison of clinical outcomes of percutaneous lumbar discectomy with DiscFX System with fenestration and decompression for contained lumbar disc herniation (LDH) with radicular pain. Chin J Pain Med. 2011; 17:31-5.
- Choy DS. Percutaneous laser disc decompression (PLDD): 12 years’ experience with 752 procedures in 518 patients. J Clin Laser Med Surg. 1998; 16:325-31.