
Impact of body mass index on acetabular anteversion
Efecto del índice de masa corporal sobre el ángulo de anteversión acetabular
O índice de massa corporal e suas consequências no ângulo de anteversão acetabular
Impact of body mass index on acetabular anteversion
Luis Enrique Martínez Manautou1,
Pamela Garza Baez2,
Ángel Eduardo Garza Moreno 1
Erick Marcelo Torres Gonzalez 1,
Judith Garza Lopez3,
Eduardo Álvarez Lozano 1
1. Hip Unit, Department of Orthopedic Surgery and Traumatology, Faculty of Medicine, University Hospital “Dr. José Eleuterio González”, Universidad Autónoma de Nuevo León (U.A.N.L). 2. Radiology Service, Faculty of Medicine, University Hospital “Dr. José Eleuterio González”, Universidad Autónoma de Nuevo León (U.A.N.L). 3. Faculty of Medicine, University Hospital “Dr. José Eleuterio González”, Universidad Autónoma de Nuevo León (U.A.N.L).
Corresponding author
Dr. Eduardo Álvarez
E-mail: contacto@dreduardoalvarez.com
Abstract
Introduction: The acetabular anteversion angle is a measurement used in computed axial tomography to evaluate acetabular morphology. Alterations in the morphology and morphometry of the acetabulum have been associated with hip pathologies. Our study aims to analyze the relationship of body mass index with femoral anteversion and establish the normal values of the acetabular anteversion angle in the Mexican population.
Material and methods: 350 patients were studied in our center between 2019 and 2020. Acetabular anteversion was measured in an axial slice of the CT scan and body mass index was calculated.
Results: A very low negative correlation was obtained for acetabular anteversion (r=-0.037) that is, the higher the BMI value, the lower the anteversion value.
Conclusion: Even though a tendency of a decreased acetabular anteversion on higher BMI classified patients was found, there is not a statistically significant relationship between BMI and acetabular anteversion angle.
Key words: Acetabular anteversion angle, body mass index, hip, pelvis, morphology
Evidence level: III
Resumen
Introducción: El ángulo de anteversión del acetábulo es una medida utilizada en tomografía axial computarizada para evaluar la morfología acetabular. Las alteraciones de la forma se han asociado con patologías de cadera. Nuestro estudio tiene como objetivo analizar la relación del índice de masa corporal con la anteversión femoral y establecer los valores normales del ángulo de anteversión acetabular en la población mexicana.
Material y métodos: Se estudiaron 350 pacientes en nuestro centro entre 2019 y 2020. Se midió la anteversión acetabular en un corte axial de TAC y se calculó el índice de masa corporal.
Resultados: Se obtuvo una correlación negativa muy baja para la anteversión acetabular (r=-0,037), es decir, a mayor valor de IMC, menor valor de anteversión.
Conclusión: Si bien se encontró una tendencia de disminución de la anteversión acetabular en los pacientes clasificados con mayor IMC, no existe una relación estadísticamente significativa entre el IMC y el ángulo de anteversión acetabular.
Key words: ángulo anteversion acetabular, Índice de masa corporal, cadera, pelvis, morfología
Nivel de evidencia: III
Introduction
The acetabulum morphology presents variability in shape, width, depth, and its diverse angulations when comparing between male and female specimens, races and during the different stages of life [1][2]. Evidence of the importance of these variations and its clinical implications during joint reconstruction and diseases such as the femoracetabular impingement, slippage of the femoral head and hip osteoarthritis has been previously described [1][3-5].
Currently, the acetabular anteversion angle is a measurement still obtained through CT scans to evaluate acetabular morphology. Its normal value varies between countries and races. Based in a study in the United States population, an average of 23°± 5°, with a range between 12° and 39° was found [6]. In a South Korean study Lim et al., [7] reported a mean acetabular anteversion angle of 17.3° in males and a 20.1° in females, while the Japanese population Maruyama et al. reported an acetabular anteversion angle of 18.5° in males and 21.3° in females [8]. In the only Mexican population study found, 118 individuals were studied with an acetabular anteversion angle average of 18.6°±4.1°, with the value in the male population 17.3°± 3.5° and 19.8°± 4.7° for women, with a range between 10°-25° and 10°-31° respectively [9].
Pelvic bone characteristics and spine morphology and its relationship with acetabular anteversion have been previously studied [1][3][5][10-12]. Sagittal morphology of the spine and pelvic tilt are coordinated to maintain balance of the limbs and for stress transmission [10]. Variations in the lateral inclination and rotation of the pelvis (pelvic tilt and spinopelvic parameters) will affect the result of the spatial orientation of the acetabulum, where anterior pelvic inclination reduces the acetabular anteversion, while the posterior inclination increases it [11].
Although weak evidence has shown that spinopelvic parameters have a direct correlation with body mass index (BMI) [13], Vargas et al., [14] concluded that the vertebral columns of obese patients present slight differences from those of the non-obese patients and therefore may affect acetabular anteversion angle. Other conclusive studies regarding BMI and acetabular anteversion were not found.
The current study was designed to assess the relationship between BMI with modifications of the acetabular anteversion angle in adult patients. As a secondary objective we opted to update the average values of acetabular anteversion in the Mexican population.
Material and methods
A retrospective, cross-sectional and descriptive study was conducted in a population of patients who had undergone abdominal or pelvic CT scan in our institution during 2019 and 2020. Inclusion criteria for patients were 18 years of age and older male and female patients, without osteoarticular pathology, history of fractures or previous pelvic, hip or lower extremity surgeries. Patients who reported the need for walking aids and /or lacked a complete institutional clinical record were excluded.
The present protocol was approved by the Institutional Review Board of the School of Medicine and University Hospital "Dr. José Eleuterio Gonzalez” of the Universidad Autonoma de Nuevo Leon with registration number: OR20-00001.
All selected patients’ weight and height were measured to calculate BMI, and were categorized in underweight, normal, overweight, grade 1 obesity and grade 2 obesity, using the formula described by Keys et al., [16][17].
The median age for the studied patients was 41 years with an interquartile range of 29 to 56 years and a range of 18 to 88 years. 41.7% (146) of the patients were male and 58.3% (204) were female. The median BMI was 26.1, with a maximum value of 38.9 and a minimum of 16.23. Most patients were concentrated in the normal weight and overweight category, only 1.1% were underweight. The demographic and clinical characteristics of the study population are described in Table 1 and Table 2.
Acetabular anteversion angle measurement
A total of 350 patients pelvic CT scans were studied, measuring their hips bilaterally with a total of 700 hips analyzed. Pelvic CT scan was performed in a neutral position, following the Visser technique [15].
Acetabular anteversion angle was measured by drawing a line in the horizontal plane through the posterior edge of both acetabula, then a second line was made perpendicular to the first one, at the level of the same posterior edge of the acetabulum for each side of the hips. Finally, a third line that runs from the anterior margin of the acetabulum to the posterior margin of the acetabulum was drawn. The acetabular anteversion angle is the measure of the angle between the second and the third lines for each side. (Figure 1)
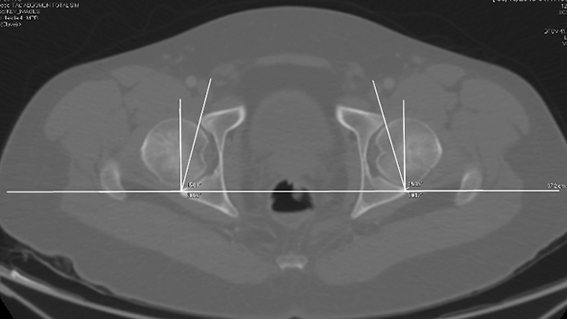
Figure 1
Statistical analysis
Categorical variables were summarized in frequencies and percentages and numerical variables in means and standard deviation. The normality of numerical variables was assessed using histograms, measures of central tendency and dispersion, and Kolmogorov-Smirnov tests. Numerical and categorical variables were compared using hypothesis tests. Pearson's Chi-Square tests were performed to look for association. Similarly, an association was sought between characteristics (numerical variables) and mortality using Student's T test for independent samples and Whitney's Mann's U test for nonparametric variables. Pearson correlation for parametric variables and Spearman's correlation for nonparametric variables were used to determine the correlation index. All statistical analyses were performed in the statistical package SPSS version 26 (IBM, Armonk, NY, USA).
Results
The average acetabular anteversion angle for men was 18.62° (18.69° and 18.59° for right and left respectively) and 21.38° for women (21.44° and 21.33° for right and left respectively) (Figure 2).
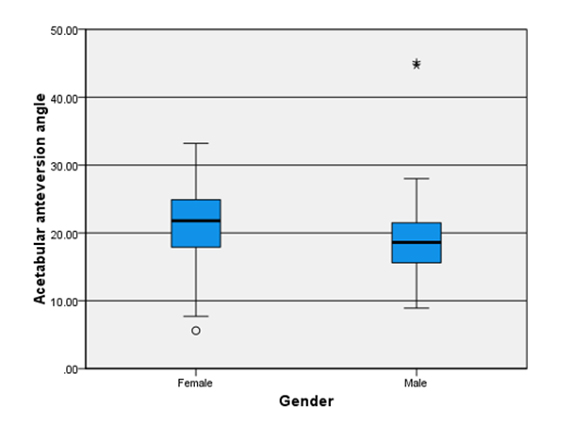
Figure 2
According to the BMI categories, the following median and interquartile range obtained was underweight 20.9 (15.8-27.3); normal 20.05(17.1-23.7); overweight 20.01 (15.4-23.6); obesity grade I, 20.8 (17.7-23.4) and obesity grade II, 18.25 (14.7-25.7) (Figure 3).
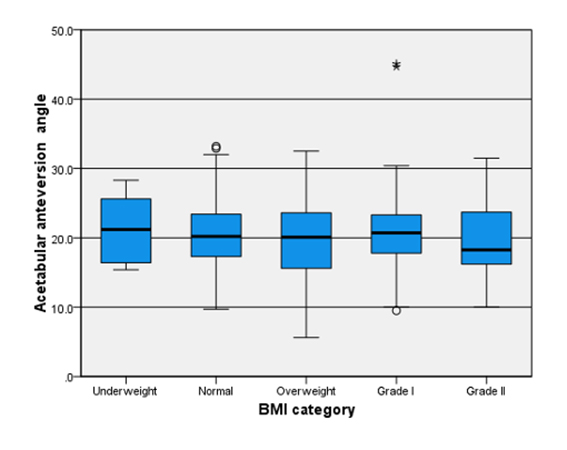
Figure 3
None of the values obtained showed statistically significant intergroup differences. A very low negative correlation was obtained for right acetabular anteversion (r = -0.042) and a very low negative correlation for the left (r = -0.032) with BMI, meaning, the higher the BMI value, the lower the anteversion value.
The results of the Pearson’s correlation between BMI and acetabular anteversion yielded very low values, being (r = -0.042) for the right side and (r = -0.032) for the left, this negative correlation indicates that the higher BMI lower the value of acetabular anteversion.
Discussion
Several relationships between BMI and hip features have been previously studied. Moran et al., [18], observed that BMI had a clinical impact in postoperative evolution of patients undergoing total hip arthroplasty. Novais et al., [3], concluded that increased BMI causes an increment in the mechanical load that falls on the hip, modifying predominantly the proximal femur morphology. Paterno et al., [20] did not found an association between the angle of acetabular anteversion and the risk of dislocation. However, even though BMI was one of the variables addressed by these authors, none of the studies described a relationship between obesity and acetabular anteversion.
One of the relevant aspects in our study was the difference in the values of the acetabular anteversion for both genders, in which men had a bilateral lower acetabular anteversion angle compared to women. This is consistent with the previous evidence described by other authors [1][2][6-9][21].
With the results obtained in this study it was not possible to demonstrate a statistically significant relationship between BMI and the angle of acetabular anteversion. Nevertheless, the number of hips measured in this study is the largest performed in the Mexican population both for male and female specimens and can be used as reference for further studies.
As limitations we considered that the CT scanner in our institution has a suggested weight limit and does not support patients over 150 kg of weight. This significantly limited the number of patients with obesity grade I, II and III for our study. We also found that the method used to measure the anteversion angle of the acetabulum its deficient. Novel forms of measuring, using 3D rendering models like the one described by Barlow et al., [22] is suggested for further studies.
Even though a tendency of a decreased acetabular anteversion on higher BMI classified patients was found, there is not a statistically significant relationship between BMI and acetabular anteversion angle. Further studies on grade II and III obesity patients are suggested.
References
- Govsa F, Ozer MA, Ozgur Z. Morphologic features of the acetabulum. Arch Orthop Traum Surg. 2005; 125:453–61.
- Krebs V, Incavo SJ, Shields WH. The anatomy of the acetabulum: what is normal? Clin Orthop Rel Res. 2009; 467:868–75.
- Novais EN, Shefelbine SJ, Kienle KP, Miller PE, Bowen G, Kim YJ, et al. Body mass index affects proximal femoral but not acetabular morphology in adolescents without hip pathology. J Bone Joint Surg (Am). 2018; 100-A:66-74.
- Menke W, Schmitz B, Schild H, Köper C. Transversal skeletal axes of the lower extremity in coxarthrosis. Zeitschr Orthop. 1991; 129:255-9.
- Jacquemier M, Jouve JL, Bollini G, Panuel M, Migliani R. Acetabular anteversion in children. J Pediatr Orthop. 1992; 12:373-5.
- Stem ES, O’Connor MI, Kransdorf MJ, Crook J. Computed tomography analysis of acetabular anteversion and abduction. Skel Radiol. 2006; 35:385-9.
- Lim C, Roh YH, Hong JE, Nam KW. Differences in Acetabular Morphology Related to Sex and Side in South Korean Population. Clin Orthop Surg. 2022; 14:486-92.
- Maruyama M, Feinberg JR, Capello WN, D’Antonio JA. Morphologic features of the acetabulum and femur: anteversion angle and implant positioning. Clin Orthop Rel Res. 2001; 393-52-65.
- Rubalcava J, Gómez-García F, Ríos-Reina JL. Angle of acetabular hip anteversion in Mexican adult population measured by computed tomography. Acta Ortop Mex. 2012; 26:155-61.
- Yang G, Li Y, Zhang H. The Influence of Pelvic Tilt on the Anteversion Angle of the Acetabular Prosthesis. Orthop Surg. 2019; 11:762–9.
- Van Bosse HJ, Lee D, Henderson ER, Sala DA, Feldman DS. Pelvic positioning creates error in CT acetabular measurements. Clin Orthop Rel Res. 2011; 469:1683-91.
- Tönnis D, Heinecke A. Current concepts review-acetabular and femoral anteversion: relationship with osteoarthritis of the hip. J Bone Joint Surg (Br). 1999; 81-B:1747-70.
- Król A, Polak M, Szczygiel E, Wójcik P, Gleb K. Relationship between mechanical factors and pelvic tilt in adults with and without low back pain. J Back Muscul Rehab. 2017; 30:699-705.
- Romero-Vargas S, Zárate-Kalfópulos B, Otero-Cámara, E, Rosales-Olivarez L, Alpízar-Aguirre A, Morales-Hernández E, Reyes-Sánchez, A. The impact of body mass index and central obesity on the spino-pelvic parameters: a correlation study. Eur Spine J. 2013; 22:878–82.
- Keys A, Fidanza F, Karvonen MJ, Kimura N, Taylor HL. Indices of relative weight and obesity. J Chron Dis. 1972; 25:329–43.
- Nuttall FQ. Body Mass Index: obesity, BMI, and health: A critical review. Nutrition today. 2015; 50:117–28.
- Visser JD, Jonkers A. A method for calculating acetabular anteversion, femur anteversion and the instability index of the hip joint. Netherlands J. Surg. 1980; 32:146-9.
- Moran M, Walmsley P, Gray A, Brenkel IJ. Does body mass index affect the early outcome of primary total hip arthroplasty? J Arthroplasty. 2005; 20:866-9.
- Deep K, Prabhakara A, Mohan D, Mahajan V, Sameer M. Orientation of transverse acetabular ligament with reference to anterior pelvic plane. Arthroplasty today. 2020; 7:1–6.
- Paterno SA, Lachiewicz PF, Kelley SS. The influence of patient related factors and the position of the acetabular component on the rate of dislocation after total hip replacement. J Bone Joint Surg (Am). 1997; 79-A:1202-10.
- Pirard E, De Lint JA. Anteversion of the acetabular component in obese patients. Hip international: the journal of clinical and experimental research on hip pathology and therapy. 2007; 17:99-103.
- Barlow KA, Krol Z, Skadlubowicz P, Dong C, Zivkovic V, Krieg AH. The "true" acetabular anteversion angle (AV angle): 2D CT versus 3D model. International journal of computer assisted radiology and surgery. 2022; 17:2337–47.
Figures
Figure 1. Acetabular anteversion angle measurement
Figure 2. Male and female acetabular anteversion angle
Figure 3. Acetabular anteversion angle and BMI categories
Table 1
Demographics of the population studied (N = 350)
|
|
N |
% |
|
Men |
146 |
41,7% |
|
Women |
204 |
58,3% |
|
Age |
41 |
29-56 |
|
Mean BMI |
26,1 |
CI 23,4 – 29,4 |
|
Anteversion angle |
20,2° |
5° |
Table 2
BMI distribution by category
|
|
N |
% |
|
Low weight |
4 |
1,1 |
|
Normal |
134 |
38,3 |
|
Overweight |
132 |
37,7 |
|
Obesity I |
63 |
18 |
|
Obesity II |
17 |
4,9 |