
Seven additional cases of polyethylene dissociation in pinnacle cup, should we start to worry?
Siete casos de disociación de polietileno en copa Pinnacle®, ¿debemos empezar a preocuparnos?
Mais sete casos de separação espontânea do polietileno do acetábulo Pinnacle®, temos de começar a preocupar-nos?
María del Coro Solans-López 1;
Esther Carbó-Laso 1, 2
Rafael Laguna-Aranda 1;
Francisco Chana-Rodríguez 1
Javier Vaquero Martín 1, 2
1- Servicio de Cirugía
Ortopédica y Traumatología. Hospital General Universitario Gregorio Marañón,
Madrid, España, 2- Departamento de Cirugía. Facultad de Medicina, Universidad
Complutense de Madrid.
Correspondencia:
Dra. M del C Soláns
Hospital General
Universitario Gregorio Marañón, Servicio de Ortopedia y Traumatología
Calle Doctor Esquerdo n° 46, 28007, Madrid, España.
Abstract
Introduction: Polyethylene
(PE) liner dissociation is an uncommon but serious complication. The Pinnacle Cup®
has shown excellent long-term results, but the number of dissociations reported
over the last five years is striking.
Methods: We
report seven cases of spontaneous dissociation of the PE liner of the Pinnacle
cup® from DePuy (Warsaw, IN, USA) occurring between 2015 and 2022. Six patients had a + 4 10° oblique insert and the
remaining one had a +4 neutral insert. Implant orientation in X-rays was
reviewed, as well as possible triggering factors and revision surgery.
Results: The mean time to dissociation
was 32 months (range, 7-60). Dissociated
PE liners showed intraoperative deformation or erosion of the rim and rupture
of 3 or 4 of the 6 anti-rotation
tabs. Ceramic insert replacement was decided in two cases,
and cup replacement was performed in the remaining five, either due to malpositioned acetabular component, or suspected damage to
the cup locking system.
Discussion: Stem
neck impingement on the PE, malorientation or excess load in the upper area of
the cups with high abduction angles, added to the lower resistance of the PE locking
system of this cup, appear to be the triggering factors in the reported cases.
The recent increase in the number of reported
cases of dissociation of the PE liner in the Pinnacle system poses the question
of the true incidence of this serious complication and the importance of
reporting it to understand the actual data.
Keywords:
Polyethylene dissociation. Pinnacle cup, Spontaneous liner dissociation, Modular acetabular components
Resumen
Introducción: La disociación
del polietileno (PE) es una complicación infrecuente pero grave. La copa Pinnacle® ha mostrado excelentes resultados a largo plazo,
pero la cantidad de disociaciones reportadas en los últimos cinco años es
sorprendente.
Métodos: Presentamos siete
casos de disociación espontánea del PE de la copa Pinnacle®,
DePuy (Warsaw, IN, EE. UU.)
ocurridos entre 2015 y 2022. Seis pacientes tenían un inserto oblicuo de +4 10°
y el restante tenía el implante +4 neutro. Se revisó la orientación de los
implantes en radiografías, así como los posibles factores desencadenantes y la
cirugía de revisión.
Resultados: El tiempo medio
de disociación fue de 32 meses (rango, 7-60). Los PE disociados mostraron
deformación o erosión intraoperatoria del borde y rotura de 3 o 4 de las 6
lengüetas antirrotación. En dos casos se decidió el reemplazo del implante de
cerámica y en los cinco restantes se realizó reemplazo de la copa, ya sea por
malposición del componente acetabular o por sospecha de daño en el sistema de
bloqueo de la copa.
Conclusión: El pinzamiento
del cuello del vástago sobre el PE, la desorientación o el exceso de carga en
la zona superior de los cotilos con ángulos de abducción elevados, sumado a la
menor resistencia del sistema de bloqueo del PE de este cotilo, parecen ser los
factores desencadenantes en lo relatado.
Palabras clave: Disociación
de polietileno. Copa Pinnacle®, disociación
espontánea del revestimiento, componentes acetabulares modulares
Resumo
Introdução: A separação do
polietileno (PE)da cúpula acetabular é uma complicação rara, mas grave. A
cúpula Pinnacle® mostrou excelentes resultados a longo prazo, mas o número de
dissociações relatadas nos últimos cinco anos é impressionante.
Métodos: Relatamos sete
casos de dissociação espontânea da cúpula de PE da cúpula Pinnacle® da DePuy
(Warsaw, IN, EUA) ocorridos entre 2015 e 2022. Seis pacientes tiveram inserção
oblíqua de +4 10° e o restante teve inserção neutra de +4 do implante. A
orientação do implante nas radiografias foi reavaliada, assim como possíveis
fatores desencadeantes de cirurgia de revisão.
Resultados: O tempo médio de
dissociação foi de 32 meses (intervalo, 7-60). As cúpulas de PE dissociados
mostraram deformação intraoperatória ou desgaste da borda e rotura de 3 ou 4
das 6 abas de anti-rotação. A substituição apenas do insert de cerâmica
foi decidida em dois casos e a de todo a cúpula acetabular foi realizada nos
cinco restantes, quer por mau posicionamento do componente acetabular quer por
suspeita de dano no sistema de travamento da cúpula.
Conclusão: O impacto do colo
da haste femoral no PE, a má orientação ou o excesso de carga na região
superior das cúpulas com altos ângulos de abdução, somado à menor resistência
do sistema de travão do PE desta cúpula, parecem ser os fatores desencadeantes
nos casos relatados.
.
Palavras-chave:
Separação do polietileno. Pinnacle
cup, Separação espontânea
do revestimento, Componentes acetabulares
modulares
Introduction:
The modularity of the acetabular
component [1] provides greater versatility and
allows for a more accurate reproduction of the patient’s hip anatomy but
introduces an additional factor of potential failure. Dissociation of the polyethylene
(PE) insert is a rare (0.17%- 2,4%) [2][3] but severe complication. Although the
Pinnacle cup® from DePuy (Warsaw, IN, USA) has shown excellent results in terms
of osseointegration and survival, attention should be drawn to the cases of PE
liner dissociation reported in recent years.
The
Pinnacle cup incorporates a Morse taper locking mechanism that allows for
implanting inserts of different materials (metallic, ceramic and PE). Previous biomechanical studies show lower resistance
to push-out and lever-out compared to other designs [4]. Moreover Perkins et al. concluded
that the lever-out strength of Pinnacle liners is shown to reduce significantly
over time compared to another commonly used acetabular system
[5].
There
are five types of PE insert in the Pinnacle system: neutral, +4 neutral
(lateralizes 4 mm the rotation centre of the hip), +4 10° (lateralizes 4mm and
changes tilt or version 10°), lipped (with an elevated rim that increases
coverage) and constrained.
We report seven cases of spontaneous dissociation
of lateralized PE inserts occurring between 2015 and 2022 at our centre, and
analyse the clinical presentation, X-rays, intraoperative findings, and most
likely mechanisms of failure.
Patients and Methods:
Patients
and surgical procedure
Five patients were women (71,42%), mean
age of the seven patients was 61.43 years (range 35-81), and mean time from
total hip replacement to revision for PE dissociation was 32 months (range 7-60).
In all patients, a total hip
prosthesis with a Pinnacle cup and a Corail or S-ROM stem were implanted. A +4 10° oblique PE insert was used in six patients, while
a +4 neutral PE insert was used in the remaining patient (Table 1). A
posterolateral approach was used. The raised rim of the oblique PE was
positioned posteroinferiorly in four patients, posterior-superiorly in one
patient and posterior in the remaining one. Hip stability and range of motion
were checked before closure, and no impingement was noted (Table 1.)
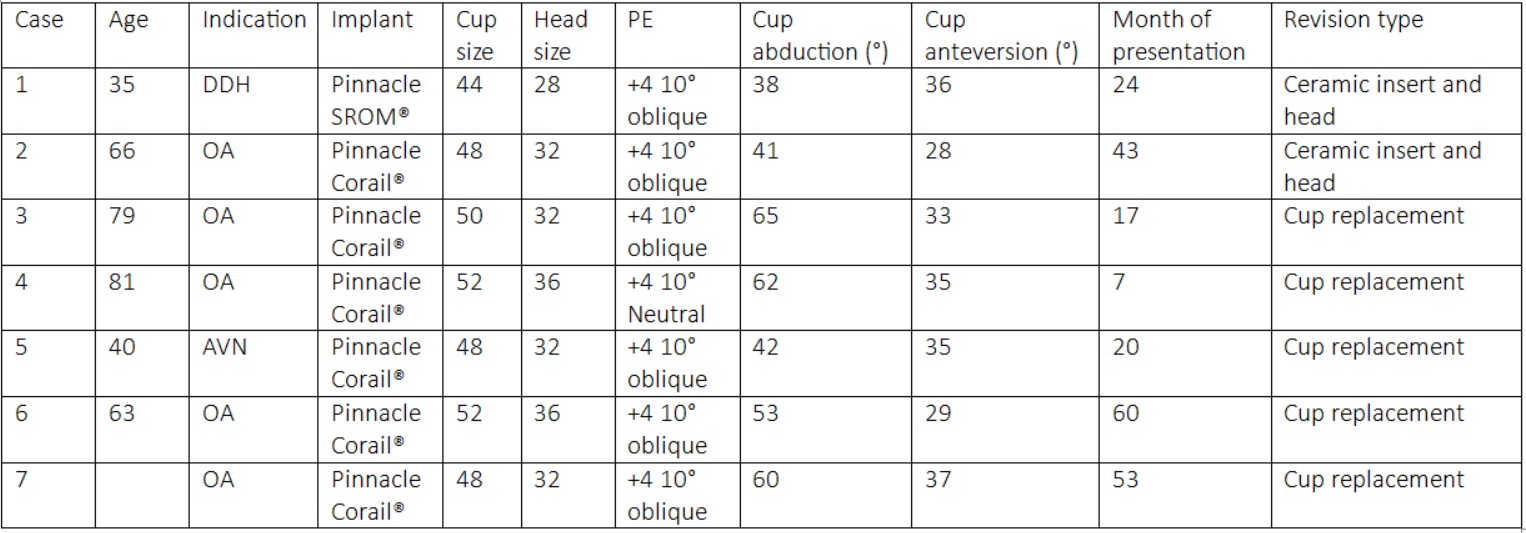
Table 1
In the informed consent forms for hip
prosthesis placement and replacement, patients authorise the use of their
clinical histories, including images, in medical publications.
Component
orientation was analysed in CT scans and plain X-rays. The method described by
Widmer [6] was
used for measuring cup anteversion. Cup tilt was calculated as the angle
between a line tangential to the acetabular component and a line joining both
tears [7].
Case reports
Case
1
A 33-year-old woman with bilateral
osteoarthritis (OA) secondary to developmental dysplasia of the hip, underwent
left hip arthroplasty (Pinnacle- S-ROM) without complications. An episode of
atraumatic anterior dislocation occurred four days after. Plain
X-rays and CT scan showed an abduction angle of the acetabular component of 38°,
a slight excess of anteversion 36° and a global offset deficiency. Revision surgery was performed, we reduced the neck stem
anteversion and increased offset using a longer head (28+3) and a lateralizad neck. The original +4 10° oblique PE was kept
posteroinferiorly.
Twenty-four months after surgery the patient
reported sudden right inguinal pain and crunching. X-rays showed an eccentric
position of the prosthetic head, and PE dissociation or rupture was suspected.
Revision surgery confirmed PE dissociation
with wear of the raised rim, suggesting impingement, and rupture of four of the
six anti-rotation tabs. The acetabular component was retained, a new ceramic insert and a 28+6 head were inserted.
Case
2
A 66-year-old woman, reported sudden
functional inability to walk accompanied by snapping on limb mobilization 43 months
after total right hip replacement (Corail,
Pinnacle cup 48, ceramic head 32, +4 10° oblique PE oriented posteroinferiorly). Radiographic
findings were consistent with PE dissociation with adequate acetabular
abduction and anteversion, 41° and 28° respectively, as measured in plain
X-rays (Figure 1) (Figure 2). During revision surgery, adequate
component orientation was confirmed. The
insert (+4 10° oblique) showed signs of wear and deformation in the
posteroinferior elevated rim, (Figure 3). The oblique insert did not provide
greater stability but caused impingement, so it was exchanged to a
ceramic insert and a 32+5 head.
Cases
3 and 4
A woman underwent total hip
replacement for bilateral hip OA at 78 and 81 years of age. Atraumatic dissociations
of the PE inserts were diagnosed 17 months after right hip replacement and 7
months after left hip replacement respectively. X-rays showed excessive cup
tilt and anteversion (right 65°/33° and left 62°/35°). The right insert was a
+4 10° oblique PE oriented postero-superiorly, and
the left a +4 neutral PE. During surgery, both
showed posterosuperior wear and rupture of the insert, and four of the six
anti-rotation tabs were broken or deformed. Both cups
were replaced, the right cup by a cemented constrained cup, and the left
cup by another Pinnacle cup with ceramic insert and head.
Case
5
A
39-year-old man underwent total hip replacement due to bilateral avascular
necrosis (AVN) of the femoral head (Corail, Pinnacle cup 48, ceramic head 32,
oblique PE oriented posteroinferiorly). 20 months after surgery, at the age of
40, he presented with a crunching sensation, without trauma. X- rays confirmed
PE dissociation, acetabular abduction angle was 42° and anteversion was 35°. In
revision surgery, we found gross metallosis, PE
dislocation with posterosuperior wear and three anti-rotation tabs broken. Cup
replacement was performed due to the suspected failure of the fixation
mechanism.
Case
6
A
58-year-old man with right hip OA underwent total hip replacement in 2017
(Corail, Pinnacle cup 52, ceramic head 36, +4 10° oblique PE oriented
posteriorly). Five years later, at the age of 63, he presented with sudden
groin pain without trauma. X- rays revealed and eccentric position of the
prosthetic head, abduction angle was 53° and anteversion was 29°. In revision
surgery we found the PE to be dislocated, posteriorly deformed and discrete metallosis. Although the components presented an
orientation at the safety limits, the hip was not stable when using a neutral
PE, so we opted to change the cup and its orientation and use a dual mobility.
Case
7
A
60-year-old-woman underwent total hip replacement (Corail,
Pinacle cup 48, ceramic head 32, +4 10° oblique PE
oriented posteroinferiorly). Six years later, at the age of 66 she reported
sudden pain and squeaking. Radiographs demonstrated subluxation of the head
superiorly within the cup, excessive abduction (60°) and anteversion (37°). We
decided to perform a cup replacement, the PE showed erosion and fracture of
three antirotation locking tabs in its upper rim.
Discussion:
PE dissociation is a very uncommon
cause of total hip replacement failure. The true incidence of this complication
is unknown. Less than 60 cases have been
reported with the Pinnacle system since the first was published in 2009 [8]. The first references to PE dissociation in a
modular cup were with the Harris-Galante 1 device (Zimmer, Warsaw, IN, USA),
and were attributed to fatigue of the insert locking mechanism [9]. Years later, the same complication, related to
possible impingement, was reported with the Harris-Galante 2 cup (Zimmer,
Warsaw, IN, USA), the Metasul cup (Zimmer, Warsaw,
IN, USA) with its metallic insert, and the tripolar Trident cup (Stryker,
Mahwah, NJ, USA).
A total of 582 Pinnacle cups with +4 neutral
or +4 10° oblique PE inserts were implanted in our institution between 2015 and
2022. The incidence of PE dislocation at our
institution between 2015 and 2022 is 1,2%. Previous authors
published rates of 0.17% in 4751 Pinnacle systems [10],
0.83% after analysing 2646 patients [2],
and 2.4% of 253 arthroplasties according to Singleton [3]. Some authors suggest that the frequency of this
complication may be underestimated because not all cases are reported.
The
anchoring system of the Pinnacle cup is a 10° Morse taper adjacent to the cup
equator for metal and ceramic inserts. To fix
the PE insert, the cup also has 12 recesses or slots in which the six
polyethylene tabs are embedded as an anti-rotation mechanism.
After conducting a systematic review
of PE dissociations, we identified 51 cases with adequate information about the
cups and PE used; Thirty-seven were
neutral PE inserts (72.55%), eleven were +4 10° oblique (face-changing)
(21.57%), two lipped (3.92%), and one +4 neutral (1.96%). The PE failed and became deformed in four patients
(7.84%), and in the remaining patients (92.16%) 3 or 4 anti-rotation tabs were
also broken [2][3][8][10-14].
Impingement is one of the proposed
dissociation mechanisms in all
types of inserts. Repeated impingement
of the stem neck on the PE rim in extreme motion positions or in patients with sagittal
spinal deformity [15]
with properly oriented cups may eventually lead to PE fatigue and deformation,
resulting in breakage of the rim and the anti-rotation tabs.
It seems logical to think that the
elevated rim of lateralized inserts may increase the risk of impingement.
However, this correlation has not been seen in the previous reported cases from
other authors, where most of the dissociated PE liners were neutral. Our seven
patients had lateralized +4 PE, in our institution we did not have neutral
inserts, we have recently introduced them for cup sizes 48 and above. Unlike
other current cups, Pinnacle system neutral PE remains elevated some
millimetres over the metallic rim, but the consequences have not yet been
analysed.
Another possible cause is inadequate
PE impaction due to soft tissue interposition or screw prominence. A decrease
in PE thickness when large heads are used in small diameter cups (as in our
cases 2,4,5,6,7) has also been suggested as a risk factor.
In
our seven patients, we think that impingement (between the stem neck and the
elevated area of the insert) and cup malposition were the factors triggering
dissociation.
In
cases 1, 2, 5 and 6 the cup was within “the safe zone” for abduction/anteversion proposed by Lewinnek et al., [16]
(Table 1) as measured by CT and AP radiographs. This constitutes a major
limitation to our study, as we
haven’t evaluated functional combined femoral and acetabular anteversion [17][18]. In revision
surgery, a +4 10° oblique trial insert (oriented as the previous one) was
tested in order to replicate the possible impingement, visually checking that
the femoral neck impacted on the elevated rim of the PE. In cases 1 and 2, we
found no gross damage to the cup locking system or significant metallosis, so we decided to change mobile parts and retain
the cup. In case number 5, the cup was changed because we found metallosis, suggesting a possible deterioration of the cup
locking system. In case number 6
the instability of the hip was the factor that made us decide to replace the
cup orientation.
In cases 3, 4 and 7, cup replacement was
performed because the primary cup was misoriented. High abduction angles (65°, 62°
and 60°) suggest that overloading the upper area of the PE-cup junction
promoted progressive PE deformation. It should be noted that time to
dissociation was shorter in cases 3 and 4, a fact already mentioned by Napier,
who stated that excessively tilted cups lead to earlier dissociation during the
first two years after surgery. We assume defects in component
orientation but believe that other systems show a much lower rate of PE
dissociation, even in the face of poorly oriented cups.
The
recent increase in the number of reports of this serious complication with the
Pinnacle system raises concern about its true incidence. Moreover, in the absence of a greater number of
dissociations reported with other systems, it seems reasonable to infer that
this system may be less permissive of surgeons’ technical errors in component
orientation. This makes us wonder, if placing an oblique face changing PE
reflects a defect in the cup orientation or hip stability. Would it not be
preferable to reorient the cup during primary surgery rather than using an
oblique PE, especially when using such a demanding system?
Dissociation
of PE in the Pinnacle cup is an uncommon complication, but we think that it
should be reported due to the widespread use of this system. Adequate cup orientation, avoiding abduction angles
greater than 50°, and careful intraoperative verification of neck-insert
impingement over wide ranges of motion should be the main factors to be
considered to decrease the incidence of this complication. Use of lateralized
PE inserts is not associated in the literature to a greater risk of dissociation,
despite being the insert used in our six patients.
References
1. Harris
WH. A New Total Hip Implant. Clin Orthop Relat Res [Internet]. 1971; 81:105–13.
Available from: http://journals.lww.com/00003086-197111000-00016
2. Yun A, Koli EN, Moreland J, Iorio R,
Tilzey JF, Mesko JW, et al. Polyethylene Liner Dissociation Is a Complication
of the DePuy Pinnacle Cup: A Report of 23 Cases. Clin Orthop Relat Res
[Internet]. 2016; 474:441–6. Available from:
http://link.springer.com/10.1007/s11999-015-4396-5
3. Singleton N. Polyethylene Liner
Dissociation with the Depuy Pinnacle Cup: A Report of 6 Cases. Orthop Res
Online J [Internet]. 2018; 3. Available from: https://crimsonpublishers.com/oproj/fulltext/OPROJ.000573.php
4. Tradonsky S, Postak PD, Froimson AI,
Greenwald AS. A comparison of the disassociation strength of modular acetabular
components. Clin Orthop Relat Res [Internet]. 1993; 296:154–60. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/8222419
5. Perkins TJ, Kop AM, Whitewood C, Pabbruwe
MB. Dissociation of polyethylene liners with the Depuy Pinnacle cup: a report
of 26 cases. Hip Int [Internet]. 2021; 11207000211008460. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/33832324
6. Widmer K-H. A simplified method to
determine acetabular cup anteversion from plain radiographs. J Arthroplasty
[Internet]. 2004; 19:387–90. Available from:
https://linkinghub.elsevier.com/retrieve/pii/S0883540303006090
7. Lu M, Zhou Y-X, Du H, Zhang J, Liu J.
Reliability and Validity of Measuring Acetabular Component Orientation by Plain
Anteroposterior Radiographs. Clin Orthop Relat Res [Internet]. 2013; 471:2987–94.
Available from: http://journals.lww.com/00003086-201309000-00038
8. Mesko JW. Acute Liner Disassociation of a
Pinnacle Acetabular Component. J Arthroplasty [Internet]. 2009; 24:815–8.
Available from: https://linkinghub.elsevier.com/retrieve/pii/S0883540308004300
9. González Della Valle A, Ruzo PS, Li S,
Pellicci P, Sculco TP, Salvati EA. Dislodgment of Polyethylene
Liners in First and Second-Generation Harris-Galante Acetabular Components. J
Bone Jt Surgery-American Vol [Internet]. 2001; 83:553–9. Available from:
http://journals.lww.com/00004623-200104000-00010
10. Napier RJ, Diamond O, O’Neill CKJ, O’Brien
S, Beverland DE. The Incidence of Dissociated Liners in 4,751 Consecutive Total
Hip Arthroplasties Using Pinnacle Polyethylene Acetabular Liners. HIP Int
[Internet]. 2017; 27:537–45. Available from: http://journals.sagepub.com/doi/10.5301/hipint.5000512
11. Kagan R, Anderson MB, Peters C, Pelt C,
Gililland J. Pinnacle polyethylene liner dissociation: a report of 3 cases.
Arthroplast Today [Internet]. 2018; 4:441–6. Available from:
https://linkinghub.elsevier.com/retrieve/pii/S2352344118300815
12. Gray CF, Moore RE, Lee G-C. Spontaneous
Dissociation of Offset, Face-Changing Polyethylene Liners from the Acetabular
Shell. J Bone Jt Surgery-American Vol [Internet]. 2012; 94:841–5. Available
from: http://journals.lww.com/00004623-201205020-00010
13. Parkar AAH, Sukeik M, El-Bakoury A, Powell
J. Acetabular liner dissociation: A case report and review of the literature.
SICOT-J [Internet]. 2019; 5:31. Available from:
https://www.sicot-j.org/10.1051/sicotj/2019025
14. Memon AR, Gwynne-Jones D. Polyethylene
liner dissociation with the Pinnacle acetabular component: should we be
concerned? Arthroplast Today [Internet]. 2020; 6:5–8. Available from:
https://linkinghub.elsevier.com/retrieve/pii/S2352344119301621
15. Yang G, Li Y, Zhang H. The Influence of
Pelvic Tilt on the Anteversion Angle of the Acetabular Prosthesis. Orthop Surg
[Internet]. 2019; 11:762–9. Available from:
https://onlinelibrary.wiley.com/doi/abs/10.1111/os.12543
16. Lewinnek GE, Lewis JL, Tarr R, Compere CL,
Zimmerman JR. Dislocations after total hip-replacement arthroplasties. J Bone
Joint Surg Am [Internet]. 1978; 60:217–20. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/641088
17. Dorr LD, Malik A, Dastane M, Wan Z.
Combined Anteversion Technique for Total Hip Arthroplasty. Clin Orthop Relat
Res [Internet]. 2009 ; 467:119–27. Available from:
http://link.springer.com/10.1007/s11999-008-0598-4
18. Kleeman-Forsthuber L, Vigdorchik JM,
Pierrepont JW, Dennis DA. Pelvic incidence significance relative to spinopelvic
risk factors for total hip arthroplasty instability. Bone Joint J [Internet].
2022; 104-B:352–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/35227099
FIGURES
Figure 1. AP Pelvis view.
Radiographic findings consistent with polyethylene dissociation. Eccentric
position of the prosthetic head. Case 2

Figure 1
Figure 2. Lateral hip view.
Radiographic findings consistent with polyethylene dissociation. Eccentric
position of the prosthetic head. Case 2

Figure 2
Figure 3. Polyethylene erosion and
deformation. Head wear. Case 2

Figure 3